Every urgent care provider knows the pressure. A parent brings in a child with an ear infection. The exam is ambiguous — it could be viral, could be bacterial. You know antibiotics probably won’t help, but the parent is expecting a prescription. You have 30 seconds to make a decision before the next patient. So you prescribe. This pattern, multiplied across thousands of encounters daily, is why 46% of urgent care antibiotics are medically unnecessary — and why antibiotic resistance is one of the CDC’s top public health threats.
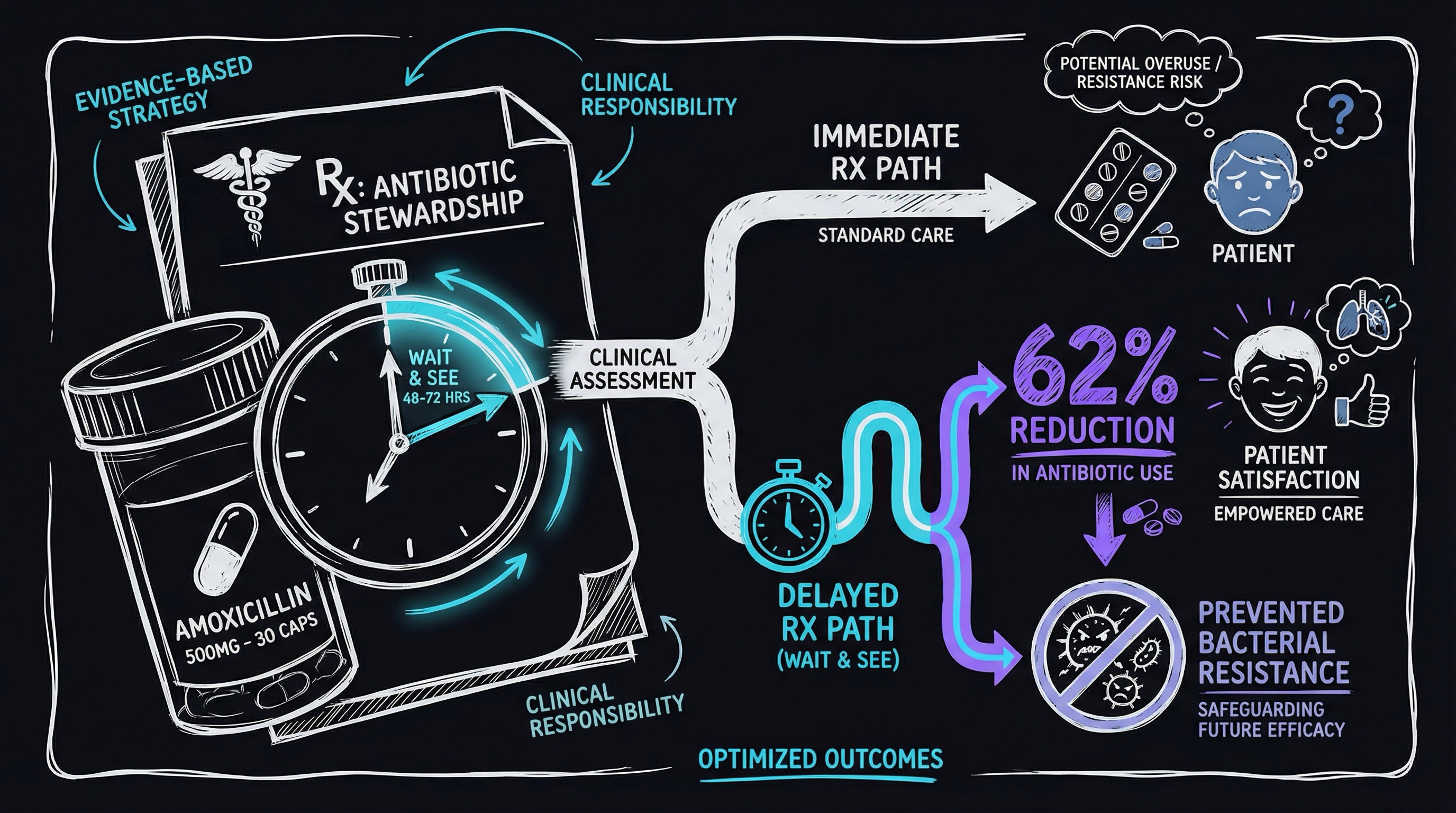
There’s a better way. The delayed prescription strategy — supported by multiple Cochrane systematic reviews and real-world implementations — achieves a 62% reduction in antibiotic consumption while maintaining 86% patient satisfaction. This isn’t theoretical. It’s evidence-based, operationally practical, and legally defensible.
The Antibiotic Pressure Problem
Urgent care exists at the intersection of patient expectations and clinical reality. Unlike primary care physicians who have longitudinal relationships with families, urgent care providers see patients once, under time pressure, with limited follow-up mechanisms. This creates several compounding pressures:
Patient expectations. Research shows that when patients expect an antibiotic, they’re significantly more likely to receive one — regardless of clinical indication. One study found that perceived patient demand increased prescribing rates by 62%, even when providers knew the infection was likely viral.
Time constraints. The average urgent care visit lasts 15-18 minutes. Explaining why antibiotics aren’t needed, addressing concerns about symptom progression, and building trust takes time that many clinics can’t afford.
Defensive medicine. Providers worry about missing a bacterial infection, particularly in pediatric cases. The fear of a complication — or worse, a malpractice claim — pushes prescribing rates upward.
Lack of follow-up infrastructure. Unlike primary care, urgent care rarely has robust systems for checking in on patients 48-72 hours later. This makes “watchful waiting” feel irresponsible.
The result? A 2018 Pew Trust analysis found that 46% of antibiotics prescribed in urgent care settings are medically unnecessary. Respiratory infections account for the majority — conditions like acute bronchitis, viral pharyngitis, and non-specific upper respiratory infections where antibiotics provide no benefit and carry real risks.
What the Evidence Shows
The delayed prescription strategy has been rigorously studied. Cochrane — the gold standard for systematic reviews — analyzed this approach across multiple studies spanning 2017-2023. The findings are compelling.
The Core Data
When providers offer a delayed prescription (with instructions to fill it only if symptoms worsen or fail to improve after 2-3 days):
- 93% of immediate prescriptions get filled (standard practice)
- 31% of delayed prescriptions get filled (delayed strategy)
- Net reduction: 62% in antibiotic consumption
Critically, this reduction comes without compromising patient outcomes:
- No increase in complications or secondary infections
- No increase in hospitalizations
- 86% of patients report satisfaction with delayed prescription approach
- Return visit rates remain stable
Why It Works Psychologically
The delayed prescription addresses the core anxieties on both sides of the exam table:
For patients: They leave with a prescription in hand — proof that their concern was taken seriously and a safety net if symptoms worsen. This satisfies the psychological need for “something to show for the visit” without requiring them to actually consume antibiotics.
For providers: They’ve ensured access to treatment if needed while avoiding unnecessary prescribing. The prescription serves as a backup plan, reducing the fear of missing a bacterial infection.
For parents: They have control. Instead of being told “just wait and see,” they’re given agency: “You’ll know in 48 hours if your child needs this. Here’s exactly what to watch for.”
The intervention works because it shifts the decision point from the high-pressure moment in the exam room to 2-3 days later at home, when the clinical picture is clearer and emotions have settled.
The Three-Tier Clinical Framework
Implementing delayed prescriptions requires clear clinical criteria. Not every infection is a candidate. Here’s the decision framework used by successful urgent care networks:
Tier 1: Immediate Antibiotics
Prescribe immediately when:
- Clear bacterial infection with high certainty (e.g., strep pharyngitis with positive rapid test)
- High-risk patient populations (immunocompromised, elderly with comorbidities, infants under 6 months)
- Severe symptoms requiring immediate treatment (high fever with systemic symptoms, spreading cellulitis, pneumonia with respiratory distress)
- Clinical indicators of bacterial etiology (purulent discharge, specific exam findings)
Clinical examples:
- Group A strep pharyngitis (positive rapid test)
- Acute otitis media in child under 2 with severe ear pain and bulging tympanic membrane
- Cellulitis with spreading erythema and lymphangitis
- Community-acquired pneumonia with consolidation on imaging
Tier 2: Delayed Prescription (The Sweet Spot)
Offer delayed prescription when:
- Clinical uncertainty exists between viral and bacterial etiology
- Mild to moderate symptoms without red flags
- Self-limiting conditions that may benefit from antibiotics only if symptoms persist beyond natural resolution timeline
- Patient or parent expresses strong desire for prescription as “backup”
Clinical examples:
- Acute otitis media in child over 2 with unilateral infection and mild symptoms
- Acute sinusitis with symptoms less than 7 days (before bacterial infection becomes likely)
- Pharyngitis with negative rapid strep test but patient worried about progression
- Uncomplicated urinary tract infection in low-risk adult with minimal symptoms
Instructions to patient:
“This is likely viral and will resolve on its own in 2-3 days. I’m giving you a prescription as a backup. Only fill it if:
- Your symptoms get significantly worse in the next 48 hours
- You’re not improving at all by day 3
- You develop new symptoms like high fever, severe pain, or spreading redness
Most patients don’t need to fill this prescription. We’ll check in with you in 48 hours to see how you’re doing.”
Tier 3: No Antibiotics
Withhold prescription entirely when:
- Clear viral etiology (acute bronchitis, viral URI, most pharyngitis)
- Conditions where antibiotics provide no benefit (viral gastroenteritis, influenza without secondary bacterial infection)
- Patient education can effectively address concerns
- Follow-up mechanisms are robust
Clinical examples:
- Acute bronchitis in otherwise healthy adult (viral 95% of the time)
- Common cold / viral URI
- Influenza (treat with antivirals if indicated, not antibiotics)
- Viral gastroenteritis
The key is being able to confidently communicate: “Antibiotics won’t help this condition and may cause side effects. Here’s what will actually make you feel better.”
Implementation Playbook
Evidence is one thing. Actually changing clinical behavior in a high-volume urgent care setting is another. Here’s how successful implementations deploy the delayed prescription strategy operationally.
1. EMR Integration: Build the Infrastructure
The delayed prescription strategy fails if it adds cognitive load or friction. It needs to be easier to do the right thing than the wrong thing.
EMR Template Setup:
Create three smart order sets in your EMR:
Template A: Immediate Antibiotic
- Standard prescription workflow
- Flags for allergy checking, dosing verification
- Patient education materials on completing full course
Template B: Delayed Prescription (the critical one)
- Prescription written but marked “Delayed - Do Not Fill Immediately”
- Auto-populated patient instructions with specific criteria for filling
- Scheduled follow-up call/text at 48 hours
- Documentation template with checkboxes for clinical reasoning
Template C: No Antibiotic
- Symptom management recommendations (hydration, rest, NSAIDs, throat lozenges, etc.)
- Red flag symptoms for return visit
- Expected timeline for symptom resolution
- Patient education materials on why antibiotics aren’t indicated
Key EMR Features:
- One-click access to all three templates from encounter screen
- Auto-documentation of clinical reasoning for delayed prescriptions (for medico-legal protection)
- Integration with pharmacy systems to flag delayed prescriptions clearly
- Automated 48-hour follow-up task creation
2. Patient Communication Materials
Waiting Room Posters:
Simple infographics explaining:
- Why most coughs, colds, and sore throats don’t need antibiotics
- Delayed prescriptions as an option
- What antibiotics actually treat (and don’t treat)
Example poster language:
“Did you know?”
- Most respiratory infections are caused by viruses
- Antibiotics don’t work on viruses
- Your body fights off most infections in 5-7 days
- Unnecessary antibiotics can cause harmful side effects and resistance
Your provider may give you a “delayed prescription” — a safety net prescription to fill only if your symptoms worsen or don’t improve in 2-3 days.
Handout for Delayed Prescriptions:
Every patient leaving with a delayed prescription receives a one-page, color-coded sheet:
🟢 GREEN ZONE (You're Improving) — Don't fill the prescription
- Symptoms are the same or getting better
- No new fever
- Energy level returning
- Eating/drinking normally
→ Continue symptom management. You're healing naturally.
🟡 YELLOW ZONE (Not Sure) — Call Us
- Symptoms not improving by day 3
- Mild new symptoms
- Unsure if you're getting better
→ Call our nurse line: [PHONE]
🔴 RED ZONE (Fill Prescription or Come Back) — Action Needed
- Symptoms significantly worse after 48 hours
- New high fever (>102°F)
- Severe pain
- Difficulty breathing or swallowing
- Spreading redness/swelling
→ Fill the prescription AND call us. If severe, return immediately.This traffic-light system makes the decision algorithm simple for patients.
3. Staff Training and Scripts
Front desk, nurses, and providers all need aligned messaging.
Front Desk Script (when patient checks in):
“Just so you know, our providers follow evidence-based guidelines on antibiotics. If your infection is viral, the provider will explain why antibiotics won’t help — but they’ll give you a plan to feel better. Sometimes they’ll give you a prescription to keep on hand, just in case.”
This sets expectations before the patient even enters the exam room.
Provider Script (in exam room):
For Tier 2 cases (delayed prescription candidates):
“I’ve examined [patient/your child] carefully. Here’s what I found: [clinical findings]. Based on this, I believe this is most likely viral, which means it will resolve on its own in 2-3 days without antibiotics.
However, I know there’s always some uncertainty with these infections. So here’s what I’m going to do: I’m writing you a prescription for an antibiotic as a backup. Don’t fill it yet. If symptoms get worse over the next 48 hours or if you’re not improving at all by day 3, then fill it and start taking it.
Most parents/patients find they don’t need to fill this prescription because their child improves on their own. But this gives you a safety net and saves you a return trip if you do need it.
We’ll also check in with you in two days to see how things are going. Does that plan make sense?”
Nurse Follow-Up Script (48-hour check-in):
“Hi, this is [Name] from [Urgent Care]. I’m calling to check on [patient] — you were seen two days ago for [condition] and given a delayed prescription. How are symptoms today?
[If improving:] Great! Sounds like you’re healing well. You don’t need to fill that prescription. Continue symptom management and call us if anything changes.
[If not improving:] Okay, it sounds like symptoms haven’t improved. Go ahead and fill that prescription and start taking it today. If you get worse or develop new symptoms, give us a call right away.”
4. Pharmacy Coordination
Alert local pharmacies that your clinic is implementing delayed prescriptions. Work with them to:
- Flag delayed prescriptions in their system so they don’t auto-fill or proactively call patients
- Add patient instructions to prescription label: “Do not fill unless symptoms worsen after 48 hours”
- Train pharmacy staff to ask: “Did your provider tell you to fill this right away or wait?” if a patient brings in a delayed prescription within 48 hours
Some EMR-pharmacy integrations allow you to set a “do not dispense before [date]” flag.
5. Quality Metrics Dashboard
Track these metrics monthly to monitor success and identify opportunities:
| Metric | Target | Purpose |
|---|---|---|
| % of respiratory infections receiving immediate antibiotics | <30% | Reduce overprescribing |
| % of respiratory infections receiving delayed prescriptions | 30-40% | Appropriate middle tier |
| % of delayed prescriptions actually filled | <35% | Confirms patient self-selection |
| Patient satisfaction scores (delayed prescription patients) | >85% | Ensure acceptance |
| Return visit rate within 7 days | Baseline | Monitor for safety signal |
| Complication rate (pneumonia, hospitalization post-visit) | Baseline | Ensure no adverse outcomes |
Set up automated monthly reports from your EMR to track these without manual effort.
Addressing Staff and Patient Concerns
Staff Concerns
“Patients will be angry if they don’t get an antibiotic.”
Reality: Studies show 86% patient satisfaction with delayed prescriptions. Patients want certainty more than antibiotics. Giving them clear criteria and a backup plan satisfies this need.
“It takes too much time to explain.”
Reality: The conversation takes 90 seconds with a good script. Compare this to the time spent dealing with an angry patient, adverse antibiotic reactions, or follow-up calls from confused patients.
“What if I miss a bacterial infection and the patient gets worse?”
Reality: The delayed prescription ensures patients have access to antibiotics if needed. Clinical decision-making is documented. You’re practicing evidence-based medicine, which is the best legal protection.
Patient Concerns
“But I always need antibiotics for these infections.”
Response: “I hear that. Many patients think their infections require antibiotics because that’s what’s worked in the past. But research shows that most of these infections resolve on their own — the antibiotics you took were just along for the ride. Let’s try this approach, and if symptoms worsen, you have the prescription ready.”
“I don’t want to come back if this gets worse.”
Response: “That’s exactly why I’m giving you this prescription now. You won’t need to come back. If you meet the criteria we discussed, you can fill this and start taking it. We’ll also call you in two days to check in.”
“I can’t afford to miss work if this doesn’t get better.”
Response: “I understand completely. That’s why this approach includes a safety net. If you’re not improving in 48 hours, you’ll start the antibiotic immediately without needing another visit. And most patients find they’re better within 2-3 days without needing the antibiotic at all.”
Metrics to Track Success
Leading Indicators (Monitor Weekly)
- Delayed prescription adoption rate — What % of eligible cases receive delayed prescriptions?
- Template utilization — Are providers using the EMR smart order sets?
- Follow-up call completion — Are 48-hour check-ins happening consistently?
Lagging Indicators (Monitor Monthly)
- Prescription fill rate — What % of delayed prescriptions are actually filled? (Target: <35%)
- Patient satisfaction — NPS or satisfaction scores for delayed prescription patients (Target: >85%)
- Antibiotic prescribing rate — Total antibiotic prescriptions per respiratory infection encounter (Target: 30-40% reduction over 6 months)
- Complication rate — Incidence of pneumonia, hospitalization, or severe adverse outcomes post-visit (should remain stable)
- Return visit rate — % of patients returning within 7 days (should remain stable or decrease)
Quality Assurance Reviews
Monthly chart audits:
- Review 10-15 delayed prescription encounters
- Verify clinical reasoning was documented
- Confirm patient received education materials
- Check that 48-hour follow-up occurred
- Review cases where delayed prescriptions were filled — were they appropriate?
Legal and Malpractice Considerations
The short answer: Delayed prescriptions are evidence-based practice and legally defensible. They reduce your malpractice risk compared to overprescribing.
Documentation Is Key
When issuing a delayed prescription, document:
- Clinical findings — Specific exam findings supporting viral etiology or clinical uncertainty
- Reasoning — “Given mild symptoms, unilateral infection, and age >2 years, delayed prescription offered per evidence-based guidelines”
- Patient education — “Patient instructed to fill prescription only if symptoms worsen or fail to improve after 48-72 hours. Provided written instructions and criteria for filling prescription. Patient verbalized understanding.”
- Follow-up plan — “48-hour follow-up call scheduled. Patient instructed on red flag symptoms requiring immediate return.”
This documentation shows:
- You performed appropriate clinical assessment
- You followed evidence-based guidelines
- You provided clear patient instructions
- You established appropriate follow-up
Legal Precedent
There is no case law showing increased malpractice liability from delayed prescribing. In fact, overprescribing antibiotics carries its own legal risks:
- Adverse reactions (C. difficile colitis, allergic reactions, drug interactions)
- Contribution to antibiotic resistance (a recognized public health harm)
- Failure to follow evidence-based guidelines (standard of care)
The CDC, American Academy of Pediatrics, and Infectious Diseases Society of America all support antibiotic stewardship strategies including delayed prescribing.
When to Consult Legal/Compliance
Before implementation:
- Review your malpractice insurance coverage — confirm that following evidence-based guidelines is covered (it always is)
- Notify your malpractice carrier of the new protocol (they’ll likely be supportive)
- Have your clinical leadership and legal team review the delayed prescription templates and patient education materials
- Ensure your EMR documentation captures the required elements
The Implementation Timeline
Month 1: Design and Approval
- Assemble stakeholder team (clinical leadership, operations, IT, quality improvement)
- Draft delayed prescription protocol with decision criteria
- Create EMR templates
- Design patient education materials
- Secure leadership approval
Month 2: Training and Pilot
- Train all clinical staff on protocol, scripts, and EMR workflow
- Pilot with 3-5 enthusiastic providers willing to test the approach
- Collect feedback and iterate on templates, scripts, and materials
- Begin tracking metrics
Month 3: Full Rollout
- Deploy to all providers
- Launch patient-facing communications (posters, website, social media)
- Coordinate with local pharmacies
- Begin 48-hour follow-up calls
- Monitor metrics weekly
Months 4-6: Optimization
- Monthly quality reviews
- Adjust templates based on provider feedback
- Share success stories and data with team
- Celebrate wins (antibiotic reduction, high satisfaction scores)
Month 6+: Sustain and Scale
- Quarterly audits to ensure sustained adherence
- Onboard new providers with standardized training
- Publish results internally to reinforce success
- Consider expanding to other infection types (UTIs, skin infections)
The Takeaway
The delayed prescription strategy is a rare win-win-win: better clinical outcomes, higher patient satisfaction, and reduced antibiotic resistance. It works because it addresses the psychological and operational realities of urgent care while staying grounded in evidence.
The barrier isn’t the science — the Cochrane reviews settled that question. The barrier is implementation: building the EMR infrastructure, training staff, creating patient materials, and tracking metrics.
But for urgent care networks serious about antibiotic stewardship, the playbook is clear. Start with the three-tier framework. Build it into your EMR. Train your team. Track your metrics. In six months, you’ll have cut unnecessary antibiotic use by more than half while maintaining the patient trust and satisfaction that keeps your clinics thriving.
The question isn’t whether delayed prescriptions work. It’s whether you’re willing to implement them.