Monday, 4:57 PM. The waiting room went from two patients to ten in under twenty minutes, and the provider who should have been seeing patient number seven was still typing the note for patient number four. By 6:30 the clinic was dead — nurses restocking rooms nobody was using. Same building, same staff, two completely different clinics inside two hours. That’s the walk-in-only model in a single shift.
Here’s what I’ve come to believe after watching this repeat: the walk-in-only model is dying, not because appointments are better medicine but because patients want to know when they’ll be seen. The clinics mixing scheduled slots with walk-in availability — the hybrid model — are dropping wait times by over 50% while pushing satisfaction to near-perfect. The fix isn’t turning people away. It’s giving them certainty.
The Problem with Walk-In-Only
Walk-in urgent care runs on demand you can’t predict. The bunching effect — patients arriving in clusters rather than a steady stream — is the whole game. Ten people at 2:00 PM buries the staff. Four o’clock is dead air.
- Long, unpredictable waits during the surges.
- Idle staff and empty rooms during the lulls.
- Frustrated patients who have no idea when they’ll be seen.
- Lower satisfaction scores despite care that’s clinically fine.
I used to assume the dissatisfaction was about clinical quality — that patients rated walk-ins lower because the medicine felt rushed. It isn’t. Research out of Ontario found that patients at walk-in clinics reported significantly lower satisfaction with their waiting experience than patients in scheduled-appointment settings — even when the clinical care was identical. Same doctor, same treatment, different wait. The wait was the whole complaint.
The Hybrid Model: Best of Both Worlds
MD Today Urgent Care, in San Diego, tried something I was skeptical of at first: they limited walk-ins to two per hour and filled the remaining slots with scheduled appointments. I worried they’d choke off the walk-in traffic that defines urgent care. They didn’t. The numbers were blunt:
- Average wait times dropped from 39 minutes (walk-ins) to 16 minutes (scheduled patients) — a 59% reduction.
- Patient ratings climbed to 4.8 out of 5 stars.
- Overall volume went up, without wait times climbing proportionally.
The insight I’d missed: scheduling doesn’t mean turning patients away. It means giving patients options — walk in now, or reserve a spot and skip the wait.
What Patients Actually Want
When patients pick an urgent care provider, the #1 factor isn’t bedside manner, insurance acceptance, or even location. It’s “appointments available right now.” That outranks everything.
- 54% of patients say online scheduling or check-in is “very important” in choosing a clinic.
- Patients who can reserve a spot come back more often than those who can’t.
- Wait-time perception — how long the wait feels — is the single largest driver of satisfaction scores.
Patients don’t just want access. They want certainty about when they’ll receive it.
Implementation: What Works
Here’s what the good hybrid operators do, based on what I’ve watched work and fail.
1. Start with Buffer Slots
Don’t kill walk-ins. Reserve 1–2 slots per hour for unscheduled patients. That keeps the urgent-care promise — come as you are — while bringing order to the rest of the day.
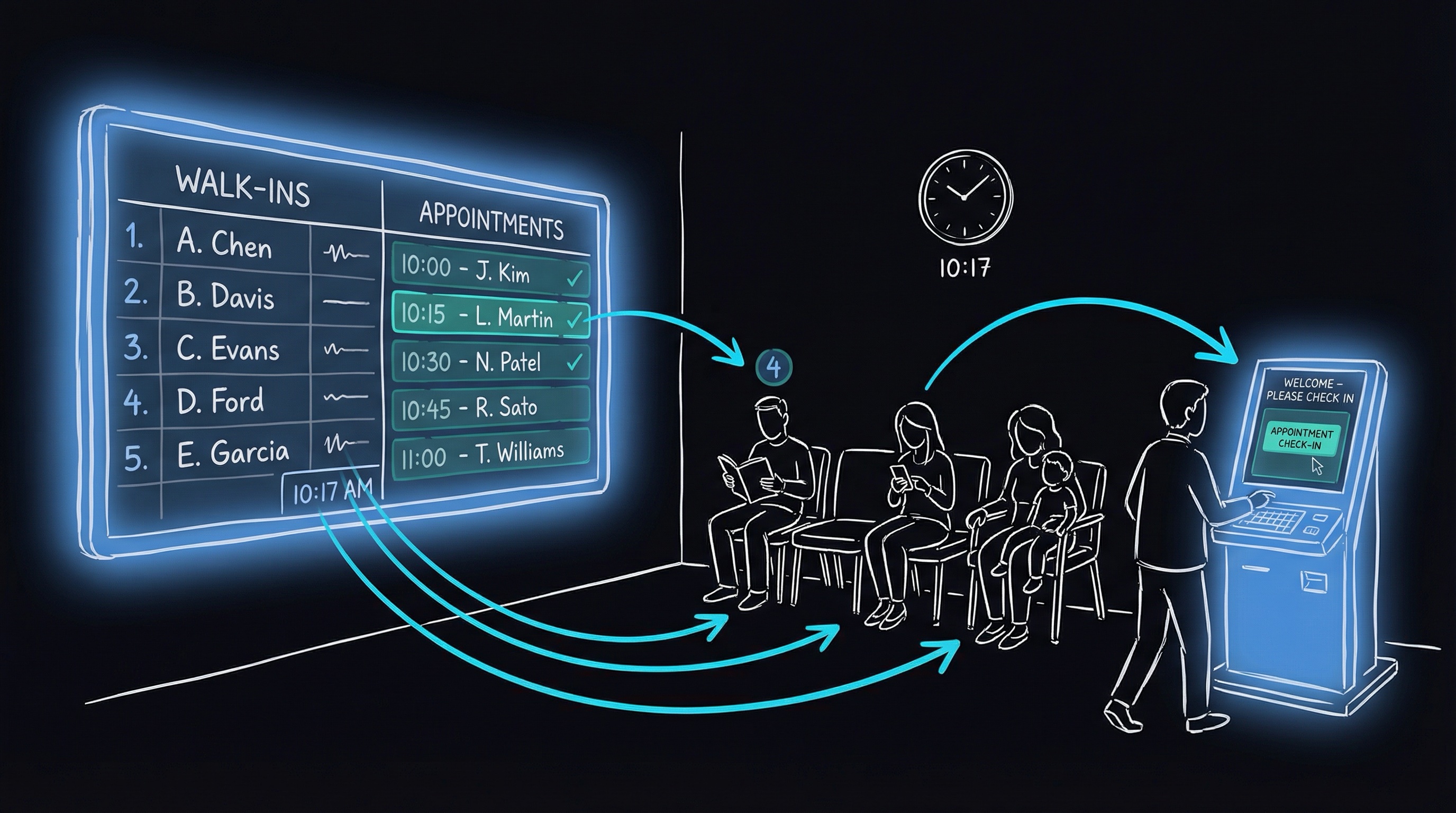
2. Deploy Digital Queue Management
Give patients a way to see their place in line. When someone can read “2 people ahead of you” or get a text when they’re next, the perceived wait shrinks fast. I used to think the problem was the minutes. It isn’t. It’s the uncertainty.
3. Train Staff on Expectation Setting
The front desk needs a consistent script: “We’ll get you in as soon as possible, but we do have some patients with reserved times this afternoon.” Empathy plus transparency.
4. Use Data to Flex the Schedule
Your own history tells you the shape of the week. Mondays at 5:00 PM are always slammed. Wednesdays at 2:00 PM are quiet. Adjust the appointment-to-walk-in ratio against those patterns instead of running one flat schedule all week.
5. Offer “Save My Spot” Virtual Queuing
The approach I underestimated isn’t a traditional appointment at all — it’s virtual waiting. The patient goes online, claims a spot in line, and arrives when their turn is close. It’s not a guaranteed appointment, but the clinic aims to start the visit within 15 minutes of arrival. For a lot of patients, that’s the sweet spot — no appointment rigidity, no lobby.
The Telemedicine Escape Valve
One pattern I’m watching closely: using telehealth — video visits — as overflow capacity. When walk-in demand outstrips what the physical clinic can handle, offer some patients a video visit right then. Patients with minor issues often prefer sorting it out on a screen to sitting in a lobby. You end up with a parallel queue — one physical, one virtual — and staff flex between them as demand shifts.
The Bottom Line
The walk-in-only model isn’t dead, but it’s no longer the default. Clinics running hybrid scheduling are seeing real, measurable gains in both operational efficiency and patient satisfaction.
The common thread: give patients certainty about when they’ll be seen, while maintaining the flexibility to handle whoever walks through the door. The operational complexity is real — I’ve watched it trip up good operators. The payoff is clearer. In a market where patients have more choices than ever, the clinic that respects their time wins.